

1) Urine routine test (urinalysis) is a test of your urine. It's used to diagnosis and monitoring a wide range of disorders, such as (UTI) urinary tract infections, kidney disease (Renal)and diabetes.
2) in the urinalysis test involves diagnosis based up on the appearance, concentration and content of urine. For example, a urinary tract infection can make urine look Hazy instead of clear. Increased levels of protein in urine can be a sign of kidney disease.
urine test used to be for monitoring for routine health.
3) A urinalysis might be part of a routine medical exam, pregnancy checkup or pre-surgery preparation. Or it might be used to screen for a various of disorders, such as diabetes, kidney disease or liver disease, when you're admitted to a hospital.
To diagnose a medical condition.
4) A urinalysis might be requested if you have abdominal pain, back pain, frequent or painful urination, blood in your urine, or other urinary conditions. A urinalysis can help diagnose the cause of these signs and symptoms.
5) urine test also be monitor a medical condition. If you've been diagnosed with a medical condition, such as kidney disease or a urinary tract infection, your doctor might recommend testing your urine regularly to monitor your condition and treatment

Specimen Collection instruction - You might be instructed to collect the urine sample midstream, using a clean-catch method. This method involves the following steps:
Cleanse the urinary opening. Women should spread the labia and clean from front to back. Men should wipe the tip of the penis.
Begin to urinate into the toilet.
Pass the collection container into your urine stream.
Urinate at least 30 ml into the collection container.
Finish urinating into the toilet.
Deliver the sample to laboratory within 60 mins.

Urine routine examination done by following three phase :
1) Physical examination.
2) Chemical examination.
3) Microscopy examination.
Physical examination : Again Physical examination analysis depends on -
i. Quantity (Volume)
ii. Color
iii. Appearance
i). Quantity (Valume)-
The urine volume depends on the amount of water excreted by the kidneys.
The volume of the urine depends upon the following:
*The fluid (water) intake.
* (water) loss from nonrenal sources.
*Excretion of dissolved solids such as glucose or salts.
* urine volume excreted indicates the balance between fluid ingestion and water loss from the lungs, sweat, and intestine.
Normal urine volume:
1200 to 1500 mL/24 hours.
The range of 600 to 2000 mL/24 hours may be considered normal.
The average urine volume is 1200 ml.
Night urine volume is usually less in amount.
The ratio of day urine to night urine is 2: 1 to 4:1.
Nocturnal polyuria:
There is increased urine at night. This may be seen in diabetes mellitus and diabetes inspidus.This may be seen as diuretics or intake of tea, coffee, or alcohol.
Polyuria is seen in:
Diabetes mellitus.Diabetes inspidus.Chronic renal disease.In the case of acromegaly.
In the case of myxedema.
Oliguria:
There is a decrease in the normal daily urine volume.Anuria or oliguria, where urine volume is <200 mL/day.This is seen in dehydration due to vomiting, diarrhea, perspiration, or severe burn.Nephritis.
Urinary tract obstruction.Acute renal failure.
Oliguria may lead to anuria.Drugs that have diuretic effects are:
Thiazides.
Alcohol.
Caffeine.
The drugs which decrease the volume and are nephrotoxic are:
Analgesics like salicylates.Antibiotics like neomycin, penicillin, and streptomycin.
ii). Color - Normal urine color is usually pale yellow to deep amber, depending on how concentrated or diluted (watery) your urine is. Cloudy urine .

For example, sperm and skin cells are harmless and could make your urine appear cloudy. Other substances that can make your urine cloudy, such as red blood cells, white blood cells and bacteria, may indicate several different medical conditions, including:
Dehydration.
Urinary tract infection (UTI).
Sexually transmitted infections (STIs).
Kidney stones.
Diabetes.
iii). Appearance : Normaly urine is Clear.
It is generally due to gross bacteriuria.
In alkaline urine, turbidity is due to amorphous phosphates and carbonates.
In acidic urine, turbidity is due to amorphous urates.
Smoky urine is due to hematuria.
In women, the epithelial cells and mucus may result in hazy urine.
2). Chemical Examination :
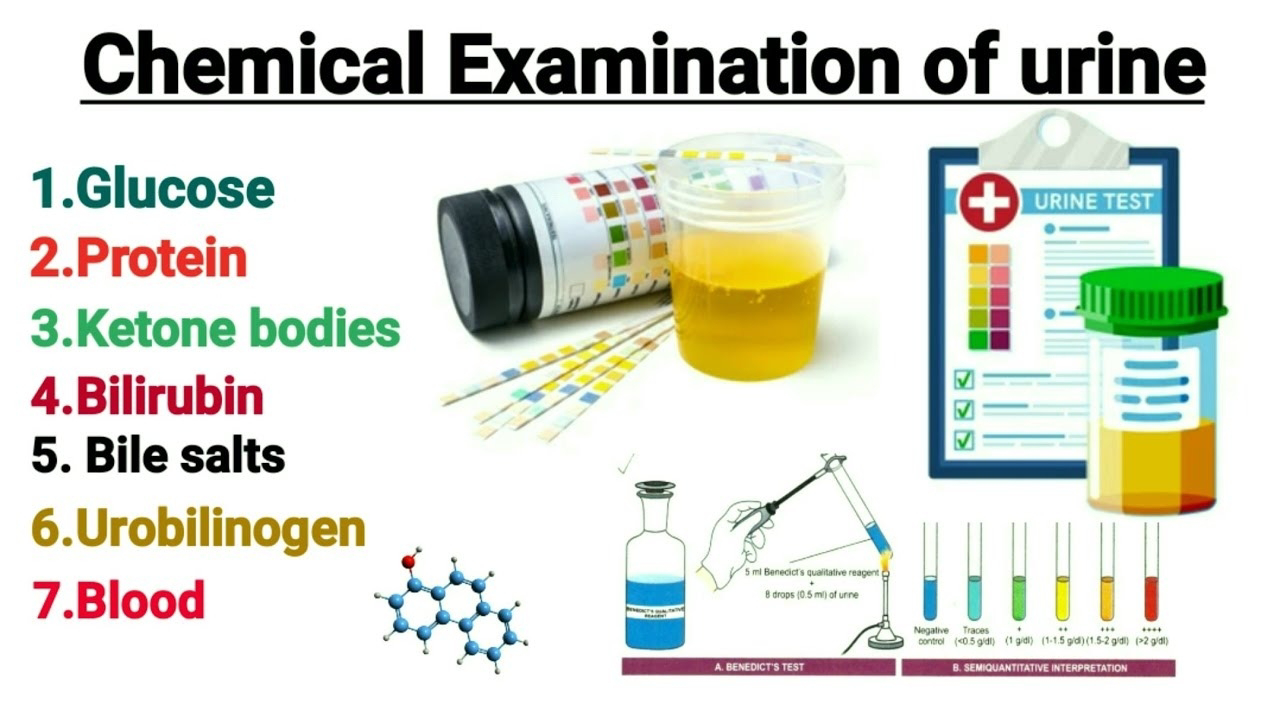
Chemical Examination for Urine Test : Commonly use Dipstick method in Laboratory, Dip the test areas of the strip in the urine specimen (fresh,well mixed and centrifuged)
Remove excess of the urine by tapping the edge of the strip against the test tube.
then the results are visually analyzed as per pack insert of urine test strip.

The result is read by visually, then cross check by chemical methods,
tests like sugar, protein, ketone and bile pigment and these results are
confirmed manually.
Following parameters are seen:
Protein
Glucose
Ketone bodies
Blood
Reaction pH
Specific Gravity
Bilirubin
Urobilinogen
Leukocytes
Nitrite

Requirement for Chemical Test :
1) Benedicts Reagent
2) 3 % Sulphosalicylic Acid
3) Barium Chloride
4) Fouchet’s Reagent
5) Sodium Nitroprusside
6) Ammonium Sulphate
7) Liquor Ammonia
8) Filter paper
9) Funnel
10) Lamp
11) glass Test tube
Manual Confirmation of Protein:
1) 3 % Sulphosalicylic acid method
Principle:
Principle is based on precipitation of protein by chemical agents (acid) or coagulation by heat.
Procedure:
• Transfer 2 ml of clear centrifuged urine to a small glass test tube.
• Add equal quantity of 3 % Sulfosalicylic acid in the specimen.
• Observe for the turbidity.

Interpretation:
• No turbidity indicates proteins absent
• Presence of turbidity indicates presence of proteins
• If proteins are present the result is graded according to the degree of turbidity as trace, 1+, 2+, 3+ & 4+.
3)Qualitative estimation of Glucose in urine:
Benedict’s method:
Principle:
When Benedict’s reagent is heated with urine, glucose present in urine reduces cupric ions present in the reagent to cuprous ions. Alkaline medium is provided to the reaction by sodium carbonate present in the
reagent. The original colour of Benedict’s reagent is blue. It changes to green, yellow, orange or red,according to the concentration of glucose present in urine.
Procedure:
• Take 5ml of Benedict’s reagent in a test tube.
• Add 7- 8 drops (0.5 ml) of urine.
• Heat carefully on the flame .
• Observe for change in colour.

Interpretation:
The change in colour of the mixture indicates the presence of glucose in urine
Green opacity, no precipitate: Present Trace
Green with yellow precipitate:
Present 1+
Yellow to green with yellow precipitate: Present 2+
Muddy orange with yellow precipitate: Present 3+
Orange or red precipitate-clear supernatant: Present 4+
4) Confirmation of ketone bodies (Rothera’s test)
Principle:
Nitroprusside reacts with both acetone and acetoacetic acid in the presence of alkali (ammonium hydroxide) to produce a purple colored compound.
Procedure:
• Take 5 ml of the urine sample in a clean dry test tube.
• Saturate the urine in ammonium sulphate.
• Add few crystals of sodium nitroprusside and shake.
• Add liquor ammonia from the side of the test tube.
• Observe for pink-purple ring at the interface.

Interpretation:
Presence of the pink-purple ring confirms the presence of ketone bodies.
• Grade the results according to the intensity of the formation of colored ring as trace, 1+, 2+, 3+ & 4+.
5) Bile Salt: Take 5 ml of urine glass tube add pinch of Sulphur powder and
check Sulphur powder is sprinkled in test tube . observe the Sulphur powder.

Interpretation:
If Sulphur powder Sink to bottom of tube, then test is positive.
Or Sulphur powder floating, then test is Negative
6) Confirmation of bile pigments:
Fouchet’s method
Dark color urine should be tested for bile pigments by Fouchet’s method
Principle:
Barium chloride reacts with sulphate radicals in the urine to form a precipitate of barium sulphate. Available bile pigments adhere to the precipitate and are detected by oxidation of bilirubin which is yellow, to biliverdin which is green, on treatment with ferric chloride in the presence of trichloroacetic acid.
Procedure:
• Take 3 – 4 ml of the urine sample in a small tube.
• Add equal amount of 10 g/dl of barium chloride.
• Mix well.
• Filter using What man No. 1 filter paper.
• Add 2 drops of Fouchet’s reagent to the sediment on the paper.

Interpretation:
Change in color to green indicates the presence of bile pigments: Positive
No change in color: Negative
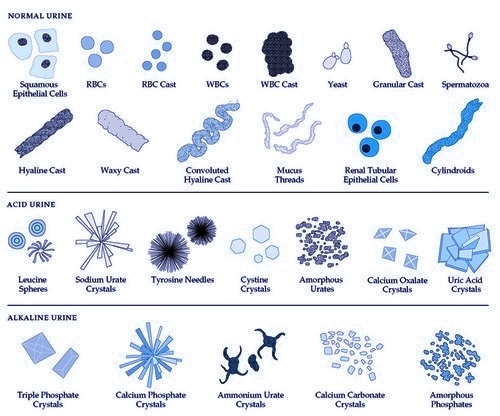
Microscope Examination:
5 ml of urine is taken in centrifuge tube and centrifuged at 2500 rpm
for 10 mins, pour off the supernatant quickly into another test tube.
The sediment at the bottom of the tube is resuspended & one drop is placed
on a clean glass slide. It is then covered with a cover slip, avoiding any air
bubbles and observed under microscope for:
1. RBC
2. Pus cells
3. Epithelial cells
4. Crystals, amorphous material
5. Casts
6. Others.








0 Comments